Anterior Cruciate Ligament (ACL) – The ultimate guide.
What is the ACL?
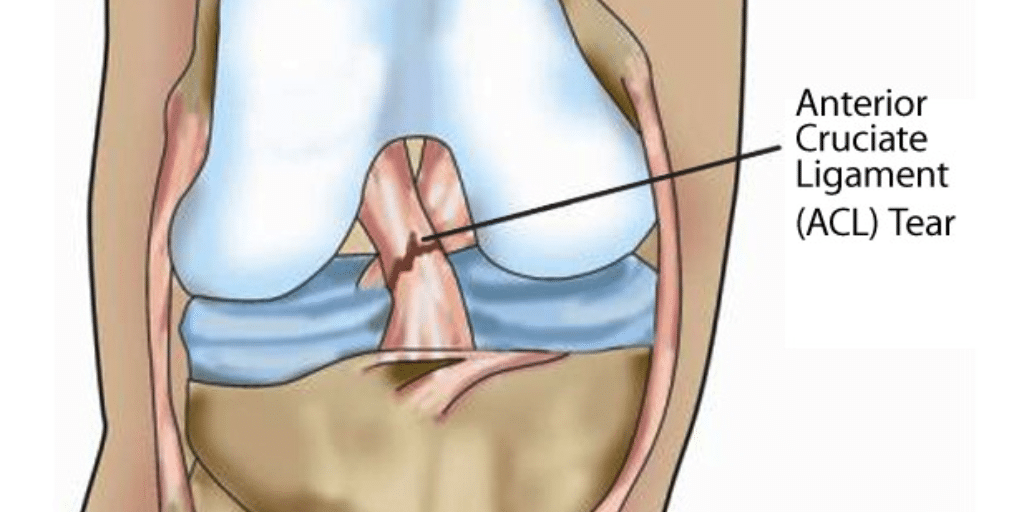
The Anterior Cruciate Ligament (ACL) is one of two ligaments (the other being the posterior cruciate ligament, or PCL) inside the knee joint which prevent excessive movement between the two bones (femur and tibia) in your knee joint. The ACL is approximately one-third the width of the PCL and correspondingly weaker, so the ACL is far more commonly injured. Without this ligament the stability of your knee is compromised.
How do you injure the ACL?
ACL injuries typically occur when twisting on a planted foot or as a result of knee hyperextension in weight-bearing. Patients describe ‘their knee going
one way and their body the other’, or that their footwear became stuck in the ground as their body kept moving, for example football boot studs being
caught in turf or a trail bike rider’s foot becoming caught in mud or a tree root.
It is quite common to hear an audible pop or crunching sound when you tear your ACL and your knee will swell very quickly1. Pain varies significantly between patients and is not necessarily an indicator of injury severity.
There are two types of ACL tears – partial tears where the ligament ends are still attached to each other and a complete rupture where the ends are completely separated 2.
ACL tears are almost always accompanied by significant bone bruising. In some cases patients may suffer a fracture or injury to other structures (ligaments or cartilage) in the knee.
How is it diagnosed?
An experienced doctor or physiotherapist can accurately assess all knee ligaments and provide an opinion regarding likely diagnosis. Hands-on tests are
most accurate either pitch-side or 1-2 weeks post-injury when pain, swelling and muscle spasm have reduced. Suspected tears are confirmed with MRI,
which is also useful in assessing damage to other structures in the knee.
How is it managed?
It is generally accepted that a complete ACL rupture will not heal itself. Your recovery therefore involves two phases – initial and ongoing management.
Initial management involves reducing the swelling and pain, this can be achieved by:
- Icing the knee for 20 minute blocks and up to 5 times a day.
- BE WARNED ICE CAN BURN so check your skin regularly to ensure it is a healthy pink, and never leave the pack on for more than 20 minutes
- Compression with a tubular bandage
- Elevating the knee for 15 minute periods as much as you can throughout the day.
- Avoiding any aggravating activities.
The ongoing management of an ACL tear depends on your age and physical goals as well as other concurrent damage to structures in your
knee. You will be referred to an orthopaedic knee specialist who will discuss management options with you3.
There are 2 main options:
- Surgical reconstruction
- Conservative management
Conservative Management
There is increasing evidence that with compliance to a specific exercise program to improve lower limb strength, flexibility and stability, many patients
with isolated ACL tears (i.e. other structures unharmed) can regain full function and return to most sporting activities. A physiotherapist can guide
you through this process, which can take up to 6 months.
However it is also thought that ACL-deficient people are at higher risk of meniscal (knee cartilage) injury with pivoting type activities, which can accelerate
development of osteoarthritis later in life. As a general rule younger people wishing to return to pivoting sports are more likely to proceed with
surgical reconstruction to regain the functional stability within the knee joint 3.
Ultimately the decision as to whether a patient should proceed with conservative or surgical management comes down to many factors, including age, activity
profile, previous or co-existing injuries and of course individual preference.
Surgical Reconstruction
This involves replacing the ruptured or torn ACL with a substitute or graft, usually part of the patient’s own hamstring tendon tissue. Over time the body
accepts this tissue as an ACL and it becomes stronger3,4. In some cases donor tissue (from another person) or an artificial ligament may
be used.

Surgery is arthroscopic (keyhole) and takes approximately one hour. Patients are in hospital overnight and are discharged the following day. Crutches are required for 1-5 days, depending on pain, and most people return to office based work within 10-14 days.
It is essential that patients see a physiotherapist post-operatively to guide them through their rehabilitation pathway. Although pain settles quickly,
the return to sport process is a long one, taking around 9-12 months. This relates to the remodelling process that takes place in the graft, whereby
maximum strength is not reached until around 9 months.
Am I at risk of rupturing my ALC again?
If a patient can regain their strength, flexibility, power and balance there is a low risk of re-injury. Research suggests re-rupture is most common in
the first 24 months post injury5 and in younger people6 (who are more likely to return to high velocity pivoting sports).
References
- Cimino, F., Volk, B. S., Setter, D. (2010). Anterior cruciate ligament injury: diagnosis, management, and prevention. American Family Physician, 82,
917-922. - Ramski, D. E., Kanj, W. W., Franklin, C. C., Keith, D. et al. (2014). Anterior Cruciate Ligament Tears in Children and Adolescents: A Meta-Analysis
of Nonoperative versus Operative Treatment. American Journal of Sports Medicine, 42 (11), 2769-2775. - Micheo, W., Hernandez, L., Seda, C. (2010). Evaluation, Management, Rehabilitation, and Prevention of Anterior Cruciate Ligament Injury: Current Concepts.
American Academy of Physical Medicine and Rehabilitation, xWilliam Micheo2(10), 935-944. - Papalia, R., Franceshi, F., Zampogna, B., Tecame, A., Mafulli, N., Denaro, V. (2014). Surgical Management of Partial Tears of the Anterior Cruciate
Ligament. Knee Surgery, Sports Traumatology, Arthroscopy, 22, 154-165. - Paterno, M., Rauh, M. J., Schmitt, L. C., Ford, K. R., Hewett, T. E. (2014). Incidence of Second ACL Injuries 2 years After Primary ACL Reconstruction
and Return to Sport. American Journal of Sports Medicine, 42(7), 1567-1573. - Kaeding, C. C., Pedroza, A. D., Reinke, E. K., Huston, L. J., Consortium, M., Spindler, K. P.(2015). Risk Factors and Predictors of Subsequent ACL
Injury in Either Knee After ACL Reconstruction. American Journal of Sports Medicine, Published online before print April 21, 2015, doi:
10.1177/0363546515578836.

Neck pain

What is Irritable Bowel Syndrome (IBS), and how can a dietitian help?

Meet Jess our new physiotherapist

Ethos Health C-fit classes

What you need to know about coffee and Health
